
Mr. C is an 89-year-old Chinese gentleman with a history of colon cancer and stage IV chronic kidney disease, who was found to have two liver masses on an abdominal CT performed without contrast. A follow-up biopsy of the larger mass confirmed that it was primary liver cancer (or hepatocellular carcinoma). But due to the lack of contrast on CT, Mr. Chen’s physicians could not rule out metastases.
Unfortunately, Mr. C was not a candidate for contrast CT because of his severe chronic kidney disease, and the high risk of further kidney failure associated with iodinated CT contrast agents. Further, since he could not hold his breath, two attempted MRI scans had severe motion artifacts and were non-diagnostic. A chest CT and bone scan did not show any extrahepatic metastasis.
Without adequate images from CT, MRI and the bone scan, physicians performed a contrast-enhanced ultrasound (CEUS) exam. Fortunately, ultrasound contrast agents are made of tiny bubbles and present no known risk of kidney damage; therefore they were safe for Mr. C.
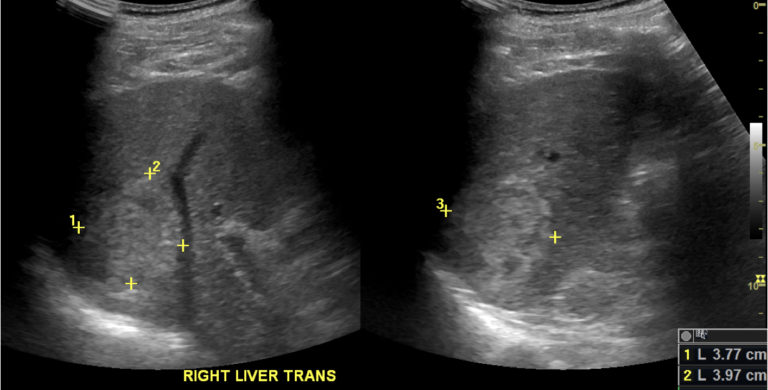
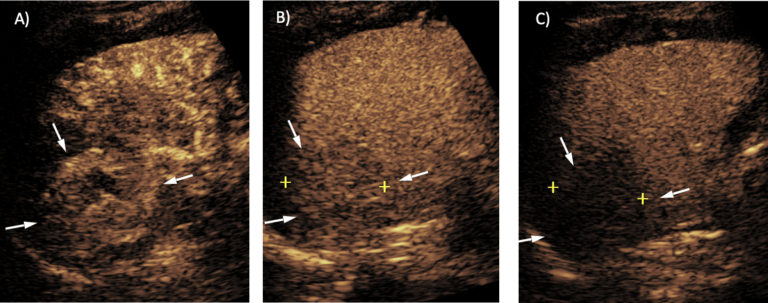
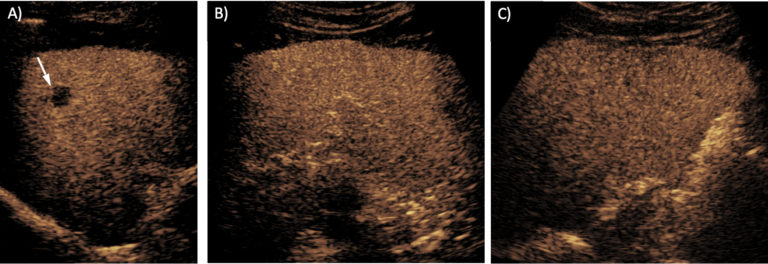
Initial gray scale images showed a 4cm hyperechoic mass in the segment 7 of the liver, and a 1.7cm cyst anterior to it. After administration of the ultrasound contrast agent, the mass showed an arterial phase hyperenhancement, with subsequent mild washout at 2 minutes — consistent with a diagnosis of HCC (CEUS LI-RADS 5). After 3 minutes, the entire liver was scanned during the portal venous phase, which confirmed no other suspicious lesion in the liver.
CEUS images provided:
These results allowed physicians to stage the disease prior to treatment, which is critical for patients with liver cancer. Thanks to the CEUS scan, Mr. C was referred to Interventional Radiology and underwent TARE (transarterial radio embolization) — a promising form of radiation therapy used to treat cancer.
Mr. C’s physicians will continue to use CEUS for ongoing post-treatment evaluations, since he cannot undergo contrast CT due to the risk of kidney damage, and he is not likely to have a good quality MRI because he cannot hold his breath.
CEUS offers an important diagnostic option when contrast CT and MRI are not helpful or available. For Mr. C, CEUS was the only feasible imaging option, and it provided good visualization of the liver. In addition, it helped rule out metastasis within the liver, which helped his physicians determine appropriate treatment.
CEUS also offers many advantages over contrast CT and MRI, including:
Superior safety profiles, especially without the risk of kidney toxicity associated with CT contrast agents, and
Performance without breath hold.
In the general population, CEUS may have limitations for HCC staging for two reasons:
CEUS is a focused exam and may not be suitable for evaluating the entire liver, and
CEUS may not be useful for assessing disease outside the liver or LN metastasis in the abdomen.
But for patients like Mr. C, CEUS is an essential imaging option, for which he and his daughter are very grateful.