Fellow Abdominal Imaging, Department of Radiology, University of Washington, Seattle, WA
Share
CEUS shows kidney mass is benign after CT suggests cancer
The ICUS Bubble Blog showcases the impact of CEUS on individual patients around the world.
Ms. B. is a young, healthy 27-year-old woman who visited a local hospital emergency room with a fever of unknown origin. Physicians there performed a routine contrast-enhanced CT scan of her abdomen and found a 2.9 cm left kidney mass (Figure 1), although they were unable to determine the source of her fever.
Figure 1 – Contrast enhanced CT axial (A) and coronal (B) views of the abdomen showed a 2.9 x 2.8 x 2.9 cm enhancing kidney mass of the upper pole (white arrows). No macroscopic fat, calcifications or scarring was seen.
The CT showed unfirmly weak contrast enhancement. CT characterization of the kidney mass would have required more radiation, which was to be avoided in this young woman since unnecessary diagnostic radiation may be associated with an increased risk of cancer that is cumulative over a patient’s lifetime.
Based on this CT, the patient’s renal mass could have been considered cancerous. Potential diagnoses included renal cell carcinoma, lymphoma and less likely non-cancerous masses such as atypical angiomyolipoma (AML). However, without adequate characterization, further evaluation was required.
Ms. B was then referred to our hospital. A conventional ultrasound (Figure 2) and contrast enhanced ultrasound (CEUS) (Figure 3) were administered to further characterize the renal mass.
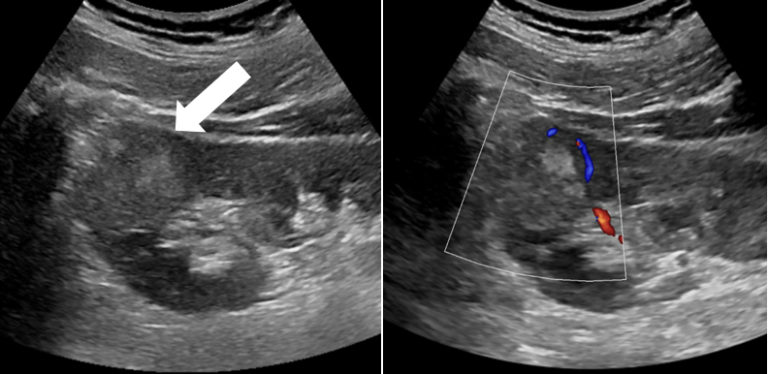
Figure 2 – Conventional ultrasound of the left kidney in long axis (A) showed a hyperechoic round mass (white arrow). Color Doppler (B) demonstrated peripheral vascularity within the mass (blue color).
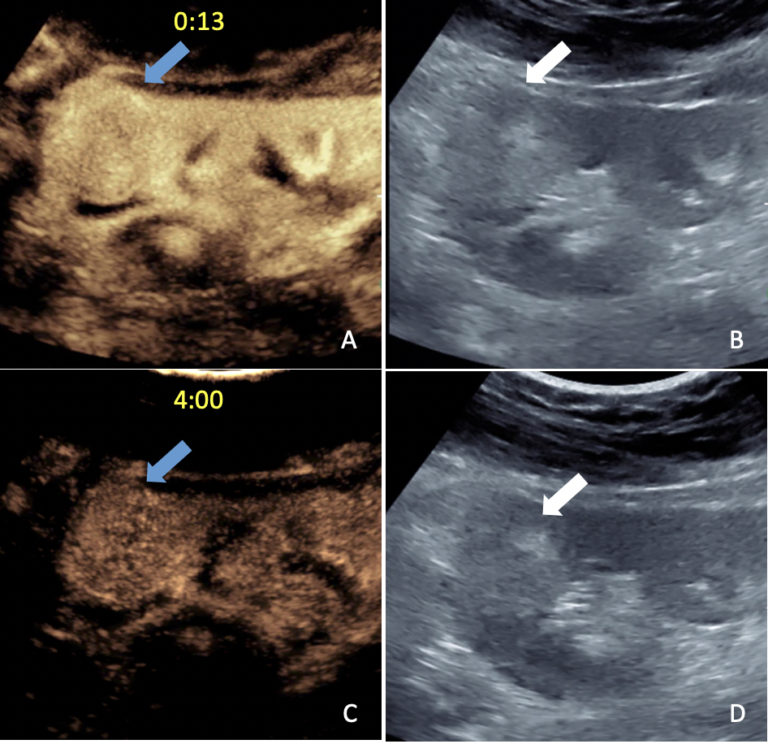
Figure 3 – Long axis contrast-enhanced ultrasound images of the left kidney with conventional mode (B, D) and ultrasound optimized to show only microbubble contrast (A, C) redemonstrated the mass (arrows). The mass enhanced early and homogenously 13 seconds after contrast injection similar to the surrounding kidney tissue (A, blue arrow). Enhancement persisted throughout the observation period. Sustained contrast enhancement more intense than the kidney was evident 4 minutes post after contrast injection (C, blue arrow).
Our CEUS imaging showed early homogenous enhancement similar to the surrounding kidney tissue, with sustained enhancement minutes after the injection. This suggested more benign etiologies such as angiomyolipoma. In addition, there was no evidence of features suggesting renal cancer or lymphoma, such as irregular enhancement or fast washout of contrast.
These encouraging CEUS results were immediately available to Ms. B, much to her relief.
An ultrasound-guided percutaneous biopsy of the mass was then performed to confirm the CEUS findings. Pathology revealed epithelioid angiomyolipoma (EAML), a rare variant of the more common AML which can mimic renal cell carcinoma on CT. Both AML and EAML are considered benign vascular tumors. Typical AMLs have intralesional fat usually seen on CT. Atypical AMLs such as EAML, may not contain fat, as in this case, and are therefore difficult to diagnose.
However, unlike AML, EAML has malignant potential and must be surgically removed. Consequently, thanks to CEUS imaging, Ms. B was able to have a robot-assisted partial left nephrectomy to remove the mass alone — and not her entire kidney.