Over the next couple of days, John underwent extensive evaluation by the surgical oncology and gastroenterology team. A follow up CT, performed approximately 30 days after the initial exam, showed improvement in the gallbladder inflammation with resolution of air in the bile ducts, but persistent gallbladder wall thickening.
To address concerns of gallbladder cancer, the radiology team was asked to perform an ultrasound-guided biopsy of the gallbladder wall. Instead the radiologist recommended a contrast-enhanced ultrasound (CEUS) scan, since CEUS is a radiation-free imaging technique and gives instant results to aid in the decision for biopsy or other management of the gallbladder wall thickening. On a CEUS scan, gallbladder cancer would enhance differently when compared to inflammatory tissues.
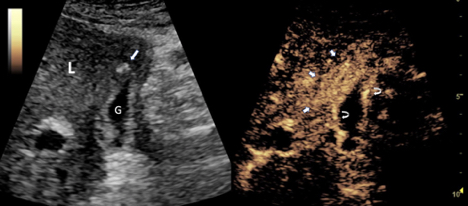
Fortunately for John, CEUS images were not consistent with cancer; rather, the CEUS scan indicated only chronic gallbladder inflammation (Figure 3,4). As a result, John was a candidate for robotic cholecystectomy — a much smaller procedure than extensive gallbladder surgery for cancer. Confirming the CEUS results, pathologic evaluation of the excised gallbladder wall showed no evidence of malignancy, but rather acute and chronic gallbladder inflammation.